Our Immunotherapy
Tumors, Tumor Immunotherapy, and Our Approach
Cancer remains one of the most pressing challenges in modern medicine. One in three individuals will be diagnosed with cancer, and one in four will die from it. This persists despite more than a century of research, involving hundreds of thousands of scientists and the publication of millions of scientific papers. Even with billions of dollars invested, a universal solution continues to elude us. Why?
Tumors arise through the malignant transformation of our own cells and often differ only subtly from healthy tissue. This similarity makes therapeutic interventions—including chemotherapy, radiation, and immunotherapy—extremely challenging. Furthermore, tumor cells exploit mechanisms embedded in our genome, originally evolved to protect germ cells and ensure species survival. For instance, tumor cells possess highly efficient defense systems against foreign substances and toxins, rendering them resistant to chemotherapy. They also deploy a variety of mechanisms to evade immune attack. Adding to this complexity is the high degree of variability among tumors. After any therapeutic intervention, surviving tumor cell subpopulations adapt and regrow more aggressively through natural selection.
There are roughly one hundred distinct tumor types, each with different stages of progression. Every tumor harbors multiple subpopulations of cells, which vary not only between tumor types but also within a single tumor. Is it even possible to develop a universally effective cancer treatment?
In 1999, Professor Zheng Cui described a remarkable discovery in mice—a spontaneous mutation known as SR/CR. This mutation endowed the mice with exceptional cancer resistance. Their immune system was capable of recognizing and eliminating various types of tumor cells. Crucially, this resistance was mediated entirely by the innate immune system—neutrophils, macrophages, and natural killer (NK) cells—that could directly identify and destroy tumor cells.
To date, the exact mechanism by which the innate immune cells of SR/CR mice recognize tumor cells remains unclear. But even if elucidated, training human innate immune cells to do the same would be a lengthy process. So, we chose a different path: to assist immune recognition directly.
Innate immune cells are particularly responsive to substances derived from bacteria, fungi, and viruses. We decided to exploit this feature by attaching such pathogen-associated molecules to the surface of tumor cells, thereby „tricking“ the immune system into recognizing the tumors as microbial threats. For this labeling, we used mannan—a component of yeast cell walls—anchored to tumor cells via BAM molecules.
To amplify the immune response, we incorporated three Toll-like receptor (TLR) agonists—resiquimod, poly(I:C), and lipoteichoic acid (LTA)—into our therapeutic mixture, which is injected directly into tumors. These molecules mimic microbial signals and recruit large numbers of innate immune cells (neutrophils, macrophages, dendritic cells, NK cells) to the tumor site. NK cells and phagocytes kill and ingest the labeled tumor cells. Phagocytes then present tumor antigens to T cells in the lymph nodes, a process enhanced by a fifth component of our mixture: an agonistic anti-CD40 antibody. This cascade leads to the generation of Th1 helper cells and cytotoxic T lymphocytes (CTLs), which eliminate residual tumor cells and metastases. Memory T cells are also formed to guard against recurrence.
Using this method, we achieve complete remission in over 80% of mice bearing advanced tumors, including melanoma, sarcoma, pancreatic adenocarcinoma, pheochromocytoma, colorectal carcinoma, breast cancer, and glioblastoma. Untreated mice typically succumb to disease within 40 days, whereas treated mice live out their normal lifespan—approximately two years—and resist re-inoculation with tumor cells.
MBTA Mechanism
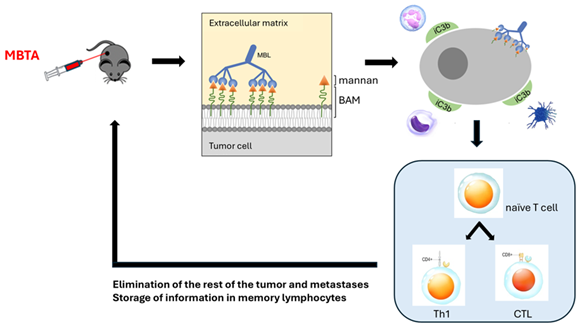
Our immunotherapeutic formula, MBTA, consists of five components: Mannan-BAM, three TLR agonists (resiquimod, poly(I:C), and LTA), and an agonistic anti-CD40 antibody. Upon intratumoral injection, mannan is anchored to the tumor cell membranes via BAM. This mannan is recognized by mannan-binding lectin (MBL), triggering complement activation and deposition of iC3b molecules on tumor cells. These opsonized cells are then targeted and phagocytosed by neutrophils, macrophages, and dendritic cells. Antigen information is relayed to T lymphocytes, which complete the destruction of tumor cells and metastases, and generate memory cells for long-term immunity.
The overall mechanism of MBTA-based tumor immunotherapy is illustrated in the figure below:
Clinical Translation
Our immunotherapy—based on the activation of innate immunity with subsequent engagement of adaptive immunity—is not specific to any tumor type. It targets tumors as a whole. However, several critical steps are needed to bring this therapy to clinical practice.
First, all therapeutic components must be produced in GMP-grade quality (Good Manufacturing Practice). Next, mandatory pharmacological and toxicological testing must be completed, even though we anticipate minimal side effects. Following these stages, the therapy must undergo the three phases of clinical trials.